I am working at my desk, writing notes in a patient’s chart, when the announcement comes: I must go to the new electronic health record (EHR) training on Friday. It is 2007, and the rise of EHRs is all over the news.
I just started working in my new job as medical director of the Aqui Para Ti /Here For You Program at the largest hospital serving a safety-net role in Minnesota — Hennepin County Medical Center, now called Hennepin Healthcare, in Minneapolis. This new innovation supports Latino teens and their families through integrative care, but confidentiality remains a central pillar of everything we do. I just learned how to navigate my life in a new job, and now I need to learn the new workaround? Oh well — the good news, they tell me, is that I have the best trainer of all!
By Friday, nerd that I am, I am all excited. The new EHR system is provided by a vendor called EPIC, and they say we are among the first to use it.
When the training ends and it’s time for questions, there I am, raising my hand, eager to learn the next step from the Master Trainer. “How do I protect adolescent confidentiality?” I ask. How many clicks will it take to make the magic happen?
The Master Trainer does not know what confidentiality for adolescents means. “Can you explain?” I do, but still doesn’t have a clue. I stare in silence. Now what?
It is now Monday. We usually see two new patients per day. At 1 pm, we see our first new patient. Let’s call her Maria. Maria is 13 years old, and in her confidential questionnaire, she shared with us that she was sexually abused when she was eight.
As she was a victim of abuse, I discuss with Maria that it is a good idea to start a contraceptive method even before being sexually active, or at least to be aware of that option. After our conversation, as she leaves (and, I guess, after she felt more trust), Maria snaps, in a typical doorknob-syndrome type of thing: “Wait! I am having sex, and I really want help. Can I have a Depo shot today?”
Mom is in the other room. EPIC is now installed on my computer, but we do not have any processes in place to place this confidential order in our new medical record. I turn around and call our department director and nurse manager; they do not know what to do, either.
I remember all the turmoil in the clinic outside Maria’s door to try to solve the issue. In the end, we offered the Depo without recording it, with our clinic’s awareness, while we continued to find an answer.
First, do not harm.
EHRs in 2007 did not anticipate the safety crisis that a violation of adolescent confidentiality can create. Reporting requirements compromised our ability to prevent, protect, and support our teen patients’ decisions and lifetime goals by providing access to confidential care.
As a member of the Society for Adolescent Health and Medicine (SAHM) since 1997 and current chair of SAHM’s diversity committee, I was trained in the importance of confidential care for teens. SAHM explained in a 2004 position paper why confidential care is essential:
- confidentiality protection is consistent with adolescent development of maturity and autonomy, and without it, some will forego care;
- confidential health care should be available to encourage adolescents to seek health care for sensitive concerns and provide complete and candid information to health care providers; and
- health care professionals should educate adolescent patients and their families about the meaning and importance of confidentiality, its scope, and its limits.
I will say that confidential care levels the field, so everyone can receive the same coaching support that parents should provide to their teens, a space to figure out what to do differently next time, a space to learn without judgment, to practice making decisions for life. But it is also true that to establish the rights for teens to have their own spaces somehow, we pushed parents out of the equation. Our mission was to do both — to solidify confidential spaces for teens in our primary care while creating awareness of the need to support parents — and to create the resources necessary to carry out that mission.
As essential hospitals, we have a “captive audience,” not by choice, but driven by the unequal forces that shape our societies. Most young people who receive Medical Assistance, Minnesota’s Medicaid program, or who have no insurance are youth of color (also referred to as minority youth, diverse youth, and nondominant ethnic and racial youth). These are the youth that Title X programs want to reach most, whom public health programs try and fail to reach. Our youth is nonmobile. We can’t tell them, “Don’t worry, go to your nearest family planning clinic, and they will fulfill your needs.” That is NOT going to happen — they don’t drive, they sometimes don’t have money for the buses, and their parents also parent in a different way: they are overprotective. (Guess what? Research says that in their environment, it works!)
What this means is that our youth is stuck with us. Literally.
We had already finished a qualitative study in which our teens talked about how they trusted us 100 percent (really), so we did not want to compromise that trust. So, in 2007, we did the unthinkable. We formed an interdisciplinary team with representatives from all parts of our hospital: labs, pharmacy, medical records, primary care departments billing, and the legal department. This team developed a unique model that brings family planning clinics to the front line of primary care clinics, where we can dispense medications to our teens directly. (Yep, with the parent sitting in a different room — usually two rooms away.)
We created what today remains the most comprehensive loophole (also known as a workflow) around EPIC to protect our teens’ access to care and rights. This workflow protects notes, labs, and medication, ensures that release of records is protected, and creates a billing mechanism so bills for those services are not sent home.
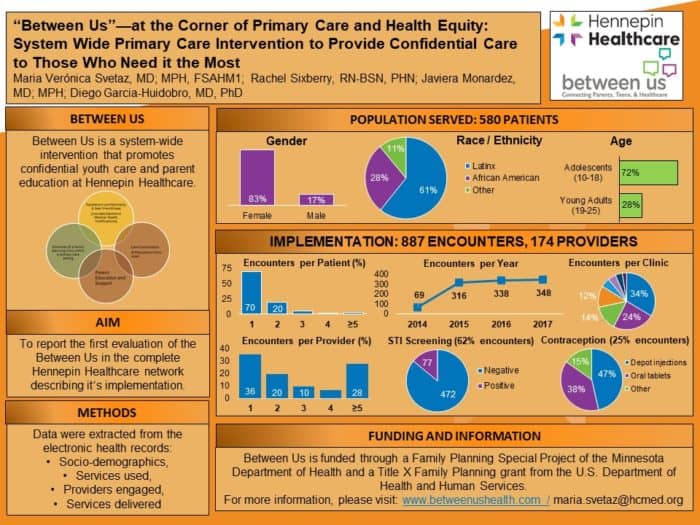
After piloting the model, then called Henne-Teen, in the same ambulatory clinic that housed our Aqui Para Ti program, we finally received a grant in 2014 through the Minnesota Department of Health’s Family Program Special Project program to expand it systemwide. We then changed the name to “Between Us” to represent the three core interventions: between youth and their providers, between parents of youth and providers, and between parents and teens.
We routinely train all our primary care workforce in how to create safe environments for both teens and parents. We conduct workshops and outreach to parents to give them the knowledge, skills, and confidence to parent positively and help their youth make sexual health decisions. We provide care coordination, which allows us to identify high-risk teens and connect them with the services needed during point-of-care at primary care clinic. We found terrific “champions” among staff throughout the process, mainly by answering honest questions about why this was a safety issue, as well as by listening to personal stories. Many staff told us “I needed something like this growing up” or “I wished you were there last year to support me coaching my teen.”
Thus far, we’ve served 580 patients through 887 encounters with 174 providers. We provided sexually transmitted infections testing to 62 percent of these patients and contraception to 25 percent of patients.
We presented our workflow at the EPIC Wisconsin Conferences in 2011 and 2015 and to the SAHM in 2017. SAHM’s 2014 recommendations for EHR use for adolescent health care are based on similar principles as our workflow.
A few months ago, writing charts after the clinic, my eyes went to the upper right corner of the EPIC screen. “What is that world icon there?” I asked myself, and, without thinking, I clicked on it (who cared, right? One more click in the midst of the hundreds per day!). A NEW world opened to me — I found an “EPIC social media” platform where users post innovations and discussions! I posted our innovation and our work in three different online “hubs”: internal medicine, family medicine, and pediatrics. Our workflow grew so much that EPIC agreed that we needed a new forum specifically for adolescent medicine to untangle the unique needs of our growing youth.
Our country’s youth have extraordinary, unique needs, highlighted by the National Academy of Medicine in its book Adolescent Health Services: Missing Opportunities. Essential hospitals like Hennepin have a critical place in serving those needs.
How many of you saw your own hospital in this story? How many of you are struggling with these same issues? The association wants to hear from you as we seek to continue supporting youth in essential hospitals. Tell us about your hospital’s work at contact@essentialhospitals.org.
Maria Veronica Svetaz, MD, MPH , is the medical director of adolescent and family medicine and director of both the Aqui Para Ti/Here for You Primary Care Behavioral Health Home for Latino Families and the Between Us task force at Hennepin Healthcare, in Minneapolis. She wants to thank the other Between Us leaders for their passion and commitment: Bibiana Garzon, Jennifer O’Brien, Rachel Sixberry, and Javiera Monardez-Popelka.